



Autodigestion?
Are powerful digestive enzymes escaping to cause the ravages of aging?

Last week, I wrote about a new study showing that in old age, the mucosal barrier thins, and digestive enzymes leak into the body and digest the tissue. Quick recap: A recent animal study showed that the thinner mucosal barrier in old age allows digestive enzymes to be absorbed into the body, where they accumulate in organs and cause tissue damage, inflammation, and, well, autodigestion.
I was left with more questions than answers, and I spent some time this week looking into digestive enzymes to see how they are made, how they can be absorbed into the bloodstream, and whether we are really digesting our own tissue with pancreatic enzymes.
To be honest, my questions aren’t the big-picture ones on digestive enzymes in old age causing autodigestion and death… Rather, I have more self-serving questions, like “Is the digestive enzyme elastase escaping the intestines and causing my crows feet?” or “Is autodigestion breaking down my joints and making me feel a bit creaky some mornings?”.
Let’s dig into the science here — and then see what we can do about it.
What are digestive enzymes?
Enzymes catalyze reactions - they make a reaction happen at a faster rate and are usually not used up in the reaction. In the body, enzymes are constantly at work in every cell, driving the cellular reactions that keep us alive.
Digestive enzymes are the specific enzymes produced to break down food into very small molecules that can be absorbed in the intestines.
Pancreatic digestive enzymes are produced in the pancreas in an inactive form and are released into the intestines where the enzymes are activated. (There are also a few other carbohydrate-digesting enzymes that are produced in the intestines, such as lactase for milk and sucrase-isomaltase for sugar.)
There are four types of digestive enzymes made in the pancreas:
Proteolytic enzymes (trypsin, chymotrypsin, elastase), which break down proteins.
Amylolytic enzymes (pancreatic amylase) - breaks down carbohydrates
Lipolytic enzymes (pancreatic lipase, prophospholipases) - break down lipids, fats
Nucleases (ribonuclease, deoxyribonuclease), which break down RNA and DNA
The combination of these powerful digestive enzymes is going to break down your dinner of steak, potatoes, and bread into absorbable fatty acids, amino acids, and smaller carbohydrates like glucose.
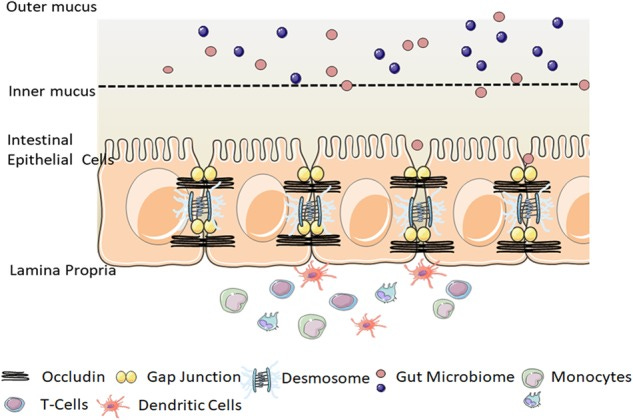
The intestinal mucosal barrier prevents the digestive enzymes from contacting the epithelial cells that make up the intestinal lining.
What happens when these enzymes come into contact with your body’s tissue?
Pancreatitis causes the circulation of pancreatic enzymes, which damages other organs:
Pancreatitis is an extreme example of what happens when digestive enzymes are released into the body.
Pancreatitis is an acute inflammation of the pancreas that is painful and potentially fatal. In pancreatitis, the enzyme trypsin is thought to be activated in the pancreas instead of in the intestines. Trypsin is a powerful digestive enzyme that breaks down protein, and it is synthesized in the pancreas as an inactive precursor form called trypsinogen. Trypsinogen is then transported to the intestine, where it is normally activated. Trypsin is important because it then activates other protein-digesting enzymes.[ref]
In pancreatitis, it is thought that the activation of trypsin in the pancreas causes the tissue of the pancreas itself to be damaged by the enzyme -- autodigestion of the pancreatic tissue. This is painful, inflammatory, and potentially releases pancreatic enzymes into the body, causing other organs to fail. For example, pancreatic lipase released in pancreatitis can cause fat tissue to break down, releasing excess non-esterified fatty acids, which then worsens organ failure.[ref][ref]
If you’re interested, you can read more about pancreatitis and genetics here.
Other conditions with damage from digestive enzymes:
Research shows that other conditions are also associated with elevated serum pancreatic enzymes.
Heart failure: A study published in July 2024 showed that serum pancreatic enzyme levels (lipase and amylase) increase significantly in acute heart failure.[ref] This adds to prior research that also showed trypsin and pancreatic lipase are significantly elevated in congestive heart failure.[ref]
Sepsis: Another study showed that about 50% of patients in the ICU with sepsis have elevated serum pancreatic enzymes (lipase and amylase).[ref]
Shock and organ failure: Animal studies show that hemorrhagic shock causes death by autodigestion. The mucosal barrier thins in shock, which allows digestive enzymes to first digest the villi and then escape into the bloodstream, lymphatic system, and peritoneum.[ref] Moreover, studies also show that neutralizing digestive enzymes in the intestines during shock can greatly reduce organ damage and inflammation.[ref]
Insulin receptors and insulin resistance: In the animal models of shock and circulating digestive enzymes, the proteases (protein-digesting enzymes) have been shown to cleave the insulin receptors on cells and cause insulin resistance.[ref]
A continual, low level of pancreatic enzymes?
To be clear, low levels of pancreatic enzymes are normal and are found in the serum of healthy individuals. The body has ways of neutralizing or dealing with this on an ongoing basis, and non-pancreatic production of some of the enzymes also occurs. In pancreatitis, high levels of pancreatic enzymes circulate, which causes damage to organs and possible organ failure.[ref][ref]
A 2006 animal study showed what happens to digestive enzymes released from the pancreas. Researchers created an animal model with fluorescently labeled amylase and lipase to see where the molecules ended up. They could see that some of the pancreatic enzymes were absorbed into the bloodstream after transcytosis across the intestinal mucosa.[ref]
The mucosal barrier:
Normally, the mucosal barrier in the gut protects the epithelial cells lining the intestines and prevents the translocation of (most) digestive enzymes into the body.
Here’s a depiction of the mucosal barrier (two layers) and intestinal epithelial cells that are held together with tight junctions:[ref]
Continual, low-level damage?
To me, the question is whether low levels of circulating digestive enzymes - or perhaps the higher end of normal levels - cause any damage to the body.
At high levels, there is definitely damage — organ failure and death. But is this a sliding scale? Do you get a little damage from the high end of the normal range of circulating digestive enzymes?
To be honest, after reading the available studies, I'm still not sure how much a constant leakage of digestive enzymes from the pancreas into the bloodstream contributes to the ongoing breakdown of the body as we age. However, if higher levels of enzymes can cause organ failure, then more moderate movement of pancreatic enzymes into the circulation and organs must be causing some damage and inflammation. Even low-level inflammation adds up and causes chronic diseases.
What decreases the intestinal mucosa?
In the studies above on organ failure and shock, a lack of blood to the intestines causes the mucosal layer to thin. So it goes without saying… avoid hemorrhagic shock. And acute pancreatitis.
The common cause of decreased mucosal barrier layer is exposure to emulsifiers and surfactants found in processed foods and medications. I think this is the key.
Let’s take a closer look at the studies on this:
Polysorbate 80:
Dating back to the early 1980s, researchers found that polysorbate 80 and polysorbate 60 (also called Tween 80, E433, or polyoxyethylene (20) sorbitan monostearate, sorbitan monooleate) thins out the mucosal barrier within 15 minutes and allows translocation of molecules through to the intestinal epithelial cells.[ref] Polysorbate 80 and 60 are used in medications to increase uptake into the body (due to mucosal thinning) and they are also used as a food ingredient.[ref]
You’ll often find polysorbate 80 in ice cream and other frozen desserts to make them smoother. It’s also found in whipped topping and pickles. Sometimes, you’ll find it in bakery items or chocolates.[ref] Hagen Dazs ice cream doesn’t have polysorbate 80, and organic pickles usually do not contain polysorbate 80. Check the ingredient labels.
Carboxymethylcellulose:
Carboxymethylcellulose (also called cellulose gum, sodium carboxymethyl cellulose, or Tylose) is a water-soluble gum that is commonly used as a thickener in foods. It may be labeled as a dietary fiber on food labels. It's also used as a detergent in laundry detergents.
Multiple animal studies clearly show that carboxymethylcellulose thins the mucosal barrier.[ref]
You’ll find carboxymethylcellulose in tortillas, sauces, dressings, candies, dairy products, and frozen foods. It is also used in pharmaceutical tablets.[ref] Again, check the ingredients.
Carrageenan:
Used as an emulsifier in many food products, carrageenan is considered a natural product because it is derived from seaweed. However, carrageenan has been shown in many studies to cause increased intestinal inflammation and decreased barrier function.[ref] I found it interesting that carrageenan is injected under the skin of lab animals to cause inflammation and swelling - used for studies on anti-inflammatory drugs.
You’ll find carrageenan in ice cream, dairy products, non-dairy creamer, milk alternatives, pudding, pie fillings, tortillas, dips, and some processed deli meats. Here’s a guide to foods that do not contain carrageenan. Note that organic foods can contain carrageenan. Check the ingredients.
In pharmaceuticals:
Surfactants are intentionally used in pharmaceuticals to increase the absorption of the drug. It is well known, though, that this causes a thinning or loosening of the mucosal barrier.[ref] This is a hard one to make recommendations on — if you need the medication and the way that it works is to degrade the intestinal mucosa, I’m not sure what your options are. If you don't need to take the medication with food, it may not matter if it temporarily thins the mucosal barrier. Of course, you could talk to your doctor to see if there are other formulations or drug options.
Increasing the mucosal barrier? Decreasing the time of digestive enzymes?
Digestive enzymes are produced in response to foods, so taking a break from eating - intermittent fasting, time-restricted eating - reduces the amount of time in which your intestines are exposed to the enzymes.
Here are a few natural options that may help increase the mucosal barrier:
Cranberry polyphenols increase gut mucosal barrier function (animal study).[ref] Here’s an example on Amazon that uses a gelatin capsule instead of a microcrystalline cellulose capsule.
Agavins, from agave, also increase gut mucosal barrier function (animal study).[ref] Agavins are found in agave. Organic agave nectar and powdered agave are readily available.
Curcumin inhibits pancreatic lipase, which may be beneficial if the mucosal barrier is compromised.
Read all about curcumin, research studies on it, and absorption.Licorice extract (Glycyrrhiza glabra) has been shown to protect the intestinal epithelial barrier function and increase the mucosal layer.[ref][ref] You can get licorice extract on Amazon, and it tastes good in tea (if you like licorice).
Inulin, which is a dietary fiber, is fermented by gut bacteria that produce short-chain fatty acids, which stimulate goblet cells to produce more mucus.[ref] You can get inulin in chicory root, garlic, Jerusalem artichokes, wheat bran, or as a prebiotic powder. If you go with the powdered form, you may want to ease into it, starting with just a small amount. Trust me on this…
* Amazon links are affiliate links, but not brand recommendations. Read the reviews and choose the best option for you. I use the credit from the affiliate links to buy more supplements for myself…
What about “leaky gut”?
The term leaky gut refers to an increased gap in the junctions between the intestinal epithelial cells. Intestinal permeability is another term, and it seems to include both the tightness of the epithelial cell junctions as well as the barrier provided by the mucosal layers. When the gap between epithelial cells gets too big, bacteria and other particles (that have made it through the mucosal barrier) are able to enter the circulation.[ref]
Research shows that endurance exercise (e.g. marathons), NSAIDs, pregnancy, and surfactants all increase intestinal permeability.[ref]
Increased intestinal permeability is associated with allergies, autoimmune diseases, depression, ALS, ME/CFS, fibromyalgia, and fatty liver disease. [ref]
What I’m not finding is any research showing that intestinal barrier function directly affects the movement of pancreatic digestive enzymes into the bloodstream. It may be that these enzymes can just as easily cross an intact intestinal epithelial barrier, and therefore leaky gut may not add much to the issue.
Conclusion:
Personally, I’m going to focus more on removing packaged foods containing emulsifiers and surfactants from my diet. Yes, this is time-consuming and essentially means making everything from scratch. A quick review of what’s in my kitchen right now shows that I need to read the labels more carefully on tortillas, cream cheese, and condiments. I’m also going to try out a few ways to increase mucosal barrier function.
Enjoy this newsletter? Please repost or share this so that I can grow the audience.
I'm wondering whether Omega 7 could play a useful role. I am allergic to fish oil, so I found a plant source that contains all the Omegas (Sea Buckthorn Oil). It has done wonders for my gut and all mucous membranes. I've only been using it for 3 months, and no more gut problems at all.
Thank you so much for writing about this. I am a subscriber to your Genetic Lifehacks and I love it. Off and on, for years I have taken Bio-zyme enzymes on an empty stomach... The thought was that as we age we have reduced amount of enzymes for repair. Now I'm totally wondering if this is a bad idea. What do you think ? I'm 75 and on no medication but I take supplements. Thank you for all your research.