

New theory of why we break down in old age: Leaking digestive enzymes cause autodigestion, tissue damage, and inflammation
Gut barrier function, emulsifiers, and digesting your own organs

I want to bring you a new study today that may answer a lot of questions about how and why we age. It’s both simple and paradigm-shifting.
First, though, let me set the stage for what happens in aging
When you zoom out and look at the big picture of aging and lifespan, one thing that stands out is the lack of progress at the end of life. Yes, the average lifespan is longer now that we have clean water and antibiotics. But why haven’t all the great medical breakthroughs over the past couple of decades moved the needle on lifespan? We have medications for everything under the sun, surgeries to fix the heart or remove cancer, stem cell therapies, biologics, cancer screenings out the wazoo, and most people stopped smoking… but this only gets us a few more years.
Here’s a chart from Our World In Data showing life expectancy by age group (to take out the effect of childhood and childbirth mortality). In the 1800s, someone who made it to their 60s or 70s was still likely to live to be close to 80. That has risen to about 85 (in England and Wales) since the 1950s with antibiotics.

Inflammation in aging:
In aging, inflammation increases, and tissues don’t work as well. It seems to be a bit of a step-function where everything in the body still works well through middle age, and then things suddenly fall apart in the later years.
We can all see the signs of aging on our skin - wrinkles, pigmentation, sagging, and thinning. Inside, the same processes are occurring, for example, in the endothelial cells lining all of our blood vessels. Research shows that inflammatory cytokines are increasing system-wide, and oxidative stress is causing cellular dysfunction…
But what is the trigger, the tipping point, the underlying cause?
Researchers led by Dr. Schmid-Schoenbein at UCSD took a new approach to the question of what causes the end breakdown in aging… and this is one study that I can’t stop thinking about.
Inflammation due to autodigestion
This new study proposes a theory of why we have inflammation, dysregulation of cell function, and a general breakdown of tissue when we get old. In a nutshell, digestive enzymes are escaping the intestines and wreaking havoc in the body by damaging tissues.
Before I go further into the animal study and the theory, I want to make clear that this is new stuff, and the experiment was mainly in rats — more research needs to be done to prove that this mechanism happens in humans at a sufficient level to drive the disease of aging.
The researchers take the view that inflammation is fundamentally to promote tissue repair, and thus there must be a mechanism in aging that causes tissue damage.
This is a unique idea that I hadn’t thought about — that there is a systemic cause of tissue damage that is driving inflammaging (inflammation as a cause of aging).
What causes tissue damage throughout the body, and then subsequent inflammation? Well, this study shows that there is a trickle of pancreatic enzymes escaping the intestines in aged animals, which causes systemic damage from autodigestion by pancreatic enzymes.
Yes - autodigestion, eating ourselves.
First, a quick overview of digestive enzymes.
When we eat, the pancreas produces a bunch of different enzymes that can break down proteins, carbohydrates, and fats from food. These include powerful protein-degrading enzymes, and if the body isn’t protected from them, the digestive enzymes can also easily break down human tissue.
Digestive enzymes are made in the pancreas in an inactive state and then released from the pancreas to be activated in the upper part of the small intestines, where specific molecules are excreted to activate the enzymes.
Just as an aside: Pancreatitis is caused when one of the pancreatic enzymes, called trypsin, is activated in the pancreas and causes autodigestion of the pancreatic tissue. This activation of trypsin and autodigestion of the pancreatic cells causes a lot of inflammation - and is very painful. Read more and learn about the genetic connections here.
Why do these powerful digestive enzymes not cause problems in the intestines? In the intestines, a mucosal layer acts as a barrier that protects the epithelial cells lining the intestines from the digestive enzymes. I always think of it as something like slug slime.
Small molecules — like micronutrients, sugars, and well-digested proteins - can pass through the intestinal barrier to be absorbed into the body. In aging, though, research shows that the permeability of the intestinal barrier shifts a little bit. Prior research shows that in people with diabetes, there is a systemic increase in proteases (protein-digesting enzymes) after a meal.
So in this new study, the scientists set out to see whether digestive enzymes are leaking into the body and at what levels. Using rats as an animal model, the researchers found that in old age there is a decrease in the barrier function of the mucosal layer. This directly led to digestive enzymes (trypsin, elastase, lipase, and amylase) leaching out of the intestines and accumulating in the organs.
The study showed that with the decreased mucosal barrier, the villi of the small intestines are infiltrated and damaged by digestive enzymes. This allows the enzymes to then travel throughout the body.
The researchers found higher levels of digestive proteases, including trypsin, amylase, and elastase, in the heart, kidney, lungs, liver, and skin in old animals, but very little or none in younger animals. One thing proteases do is break down collagen and the extracellular matrix, which is a big problem for lung function as well as in blood vessels.
Here’s an image from the study (open access, go read it):
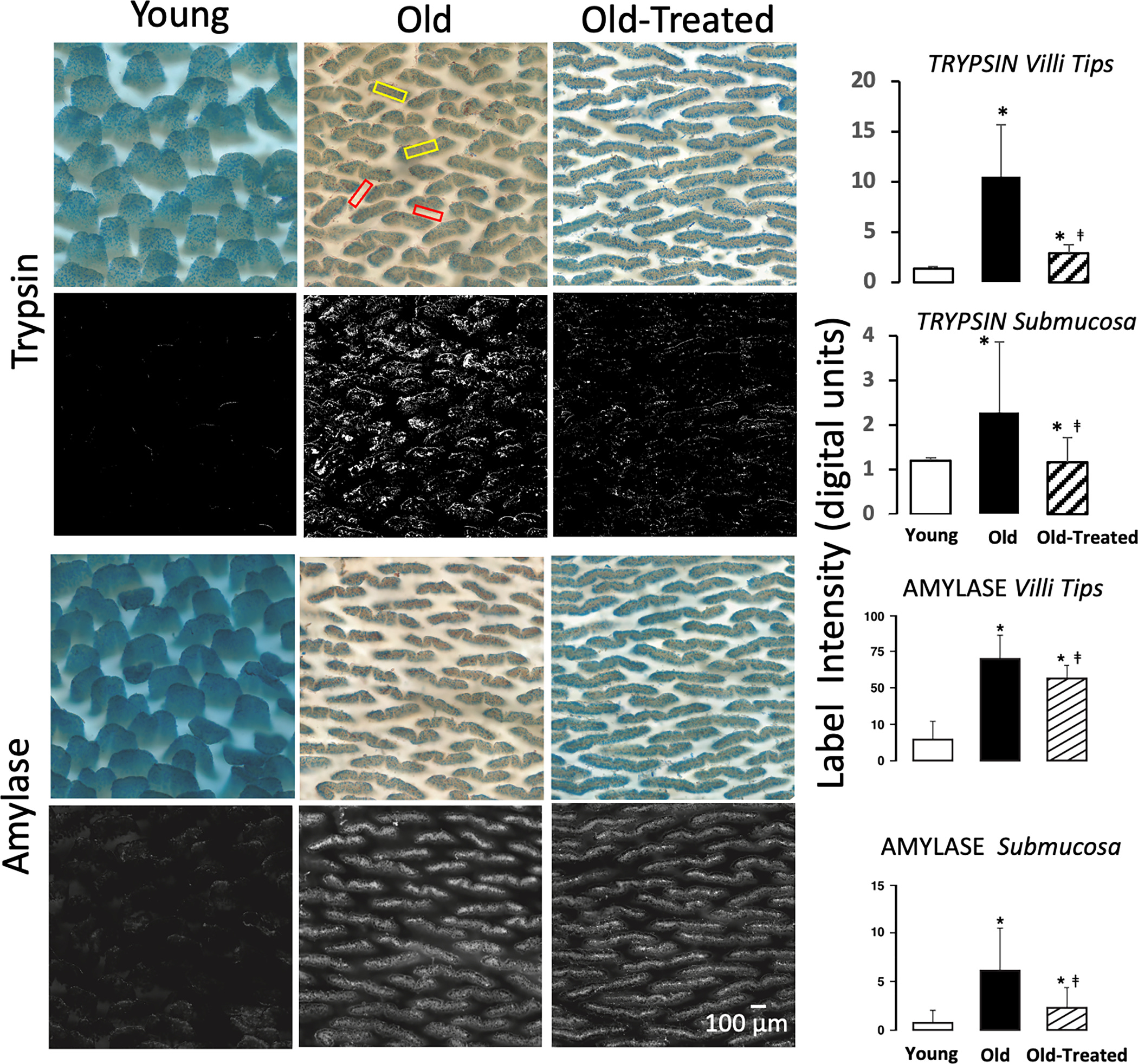
The accumulation of digestive enzymes in the organs causes tissue damage, which then triggers inflammation (likely starting a cascade of more damage).
The liver also produces enzymes that inactivate the pancreatic digestive enzymes, so it is a tipping point where the liver isn’t keeping up with the ability to balance out any escaped digestive enzymes.
Importantly, this can be partially reversed:
The researchers showed that giving the old rats a pancreatic trypsin inhibitor reduced the accumulation of digestive enzymes in the organs and also helped protect the mucin barrier from breakdown. The researchers used tranexamic acid as the trypsin inhibitor. Tranexamic acid is a prescription medication used to increase clotting by blocking the breakdown of clots, so it isn’t something that everyone should use as an anti-aging supplement.
However, there may be other ways to prevent the breakdown of the mucosal barrier in the intestines.
Let’s look at some possible solutions here (keeping in mind that this is speculation and experiments need to be done)…
Ways of improving the gut mucosal barrier:
First, let’s look at why the mucosal barrier may be thinned out, and then a couple of ways that you can increase the mucosal layer.
Emulsifiers in processed foods cause intestinal mucosal thinning:
Studies dating back a decade or more show that emulsifiers and surfactants in processed foods can thin the intestinal barrier.[ref]
Emulsifiers and surfactants essentially act like adding a drop of Dawn to a greasy pan — or using soap to break down something slimy, like the gut mucosal barrier. That’s their job, but emulsifiers and surfactants are now added to many processed foods to improve shelf stability and texture.
Carboxymethylcellulose and polysorbate 80 are two of the well-studied emulsifiers that are known to thin the mucosal layer.
Drug manufacturers use this same mucosal thinning property and include surfactants in many medications. Look for polysorbate 80, tween 80, polysorbate 20, and carboxymethylcellulose. All of these things thin the intestinal mucosa so that more of the drug can be absorbed into the body.
Not everyone has the same reaction to carboxymethylcellulose or polysorbate 80. For some people with genetic variants in NOD2 or IL-10, these emulsifiers will cause an immune system reaction due to the translocation of bacteria when the mucosal barrier is thinned. Here’s the Genetic Lifehacks article on emulsifiers and leaky gut.
For others, research shows that it isn’t genetics but rather the composition of the gut microbiome that drives intestinal inflammation due to emulsifiers.[ref]
Surfactants in medications:
Pharmaceutical manufacturers figured out that medications work better if they are more readily absorbed in the intestines. So some medications deliberately include polysorbate 80, polysorbate 20, or carboxymethylcellulose to help with absorption. [ref][ref] Here’s a list of tablets containing CMC and medications containing polysorbate 80.
Alcohol acts on the mucosal barrier:
Alcohol can also act as a surfactant and increase the permeability of the intestines. There are thousands of studies showing that alcohol temporarily reduces the mucosal barrier.[ref]
Increasing mucin:
What about increasing the production of mucin and increasing the mucosal barrier function? Here are several natural substances that promote an increase in the mucosal barrier.
Flavonoids in licorice increase the regeneration of mucin-producing cells and also increase the mucosal barrier.[ref]
Glutamine is well known for improving the mucosal layer.[ref]
Animal studies show that bee propolis increases the intestinal mucosal barrier. [ref]
Vitamin A is important in intestinal barrier function. For someone who is vitamin A deficient, increasing vitamin A intake should promote the mucosal barrier.[ref]
Zinc carnosine has been shown to stabilize the gut mucosal barrier.[ref]
Questions that I still have (for a follow-up article next week):
Reducing production:
Since we release digestive enzymes in anticipation of eating, would time-restricted eating, intermittent fasting, or one meal a day (OMAD) help with reducing the burden of digestive enzymes escaping into the body? Is this why calorie-restricted diets increase longevity for mice?
ROS in the intestines:
A very cool study in 2020 showed that sleep deprivation kills us by increasing oxidative stress in the intestines. It wasn’t leaky gut or bacteria in the bloodstream, but rather just oxidative stress that increased with lack of sleep and caused death. Is there a link there to the thinning of the mucosal barrier and autodigestion?
Pancreatic enzyme supplements:
Do supplemental digestive enzymes cause problems in people with decreased mucosal barrier function?
Alpha-1 antitrypsin:
The body produces an enzyme called alpha-1 antitrypsin that neutralizes trypsin, proteinase 2, caspase 3, chymase, and elastase. Alpha-1 antitrypsin is predominantly made in the liver and then transported to the lungs. Elastin in the lungs is important for keeping them flexible, and elastase can break that down. Thus, alpha-1 antitrypsin is important because it deactivates elastase before it damages lung cells. Mutations that cause changes in alpha-1 antitrypsin eventually cause COPD due to a lack of elastase neutralization in the lungs and liver problems due to the enzyme being stuck in the liver.
Fat in the diet:
How does the amount of dietary fat affect digestive enzymes?
I’ll keep digging into the research and come back with more answers next week.
» edit: Here’s the next article on this topic »
Want to learn more? I just found a great podcast with the author of the study. In it, he goes into some interesting points that aren’t in the study and raises a lot more questions that I didn’t think of.